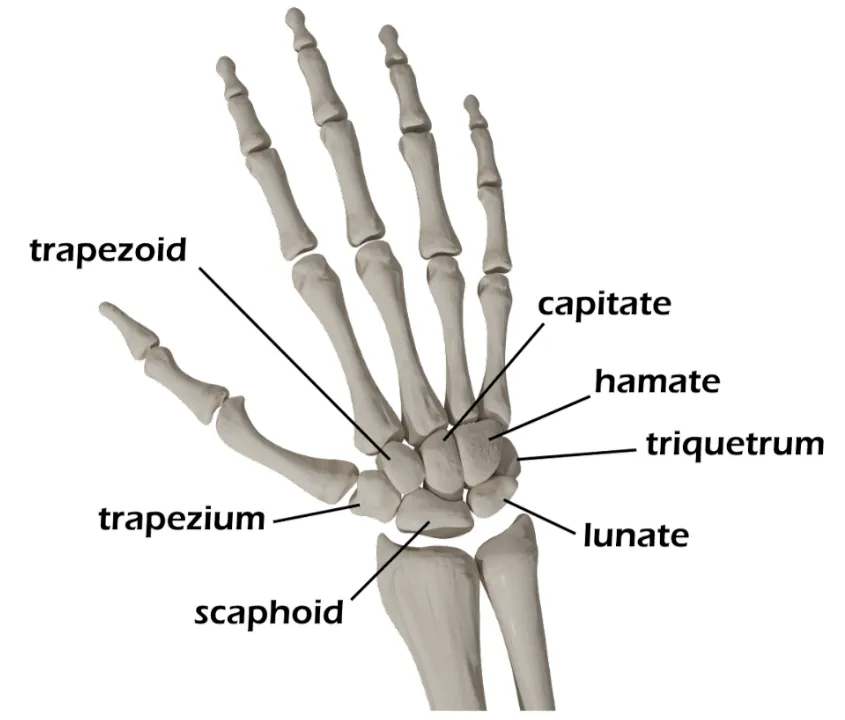
Trapezium Fracture
- Rare fracture - approximately ~1% of all carpal fractures
- Often occurs from axial loading mechanism to the 1st metacarpal or wrist
- Vast majority of these fractures can be immobilized in an thumb spica splint and discharged with orthopaedic follow up
- Mechanism
- Axial loading of the thumb
- Axial loading of the wrist
- Timing of injury
- Other locations of pain/Associated injuries
- Often accompanied by fracture at the base of the 1st metacarpal
- May co-occur with scaphoid, captitate, and trapezoid fracture
- Numbness/tingling
- Hand dominance
- Profession
Vitals
- Swelling about the volar base of the thumb
- Pain with palpation and axial loading of the first metacarpal
- Poke holes or punctate wounds → open injuries
- Dorsal wounds are commonly open fractures
- Do not miss this; if seen, give IV cefazolin (2-3g) immediately
Motor Exam:
- Median Nerve/ Anterior interosseous nerve (AIN)
- Opposition of the thumb
- Opponens innervated by the median nerve - helpful to assess if concern for acute carpal tunnel syndrome
- Flexion of wrist, fingers, thumb
- “A-OK sign” = AIN
-
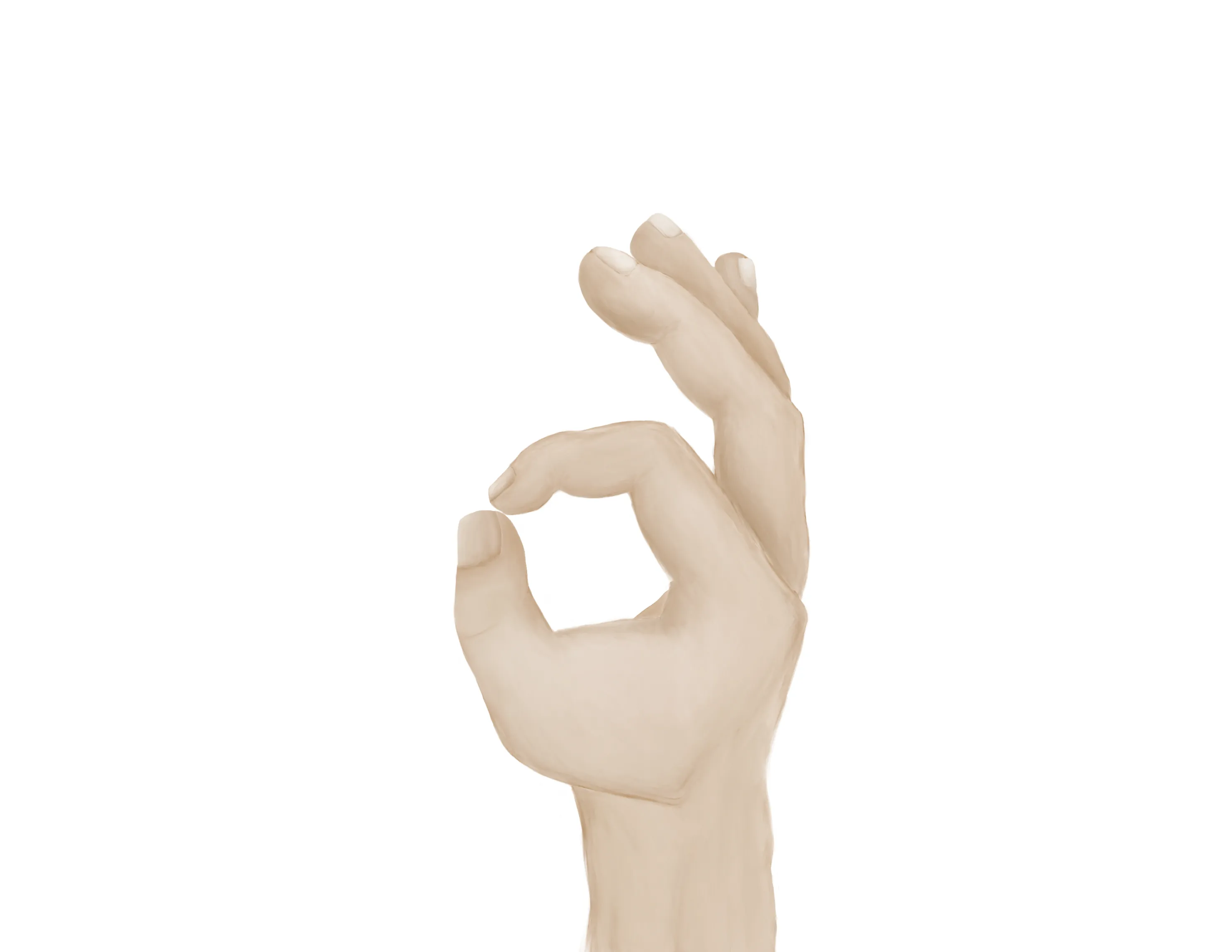
- Tests flexion of thumb IP joint (FPL) and flexion of index DIP joint (FDP)
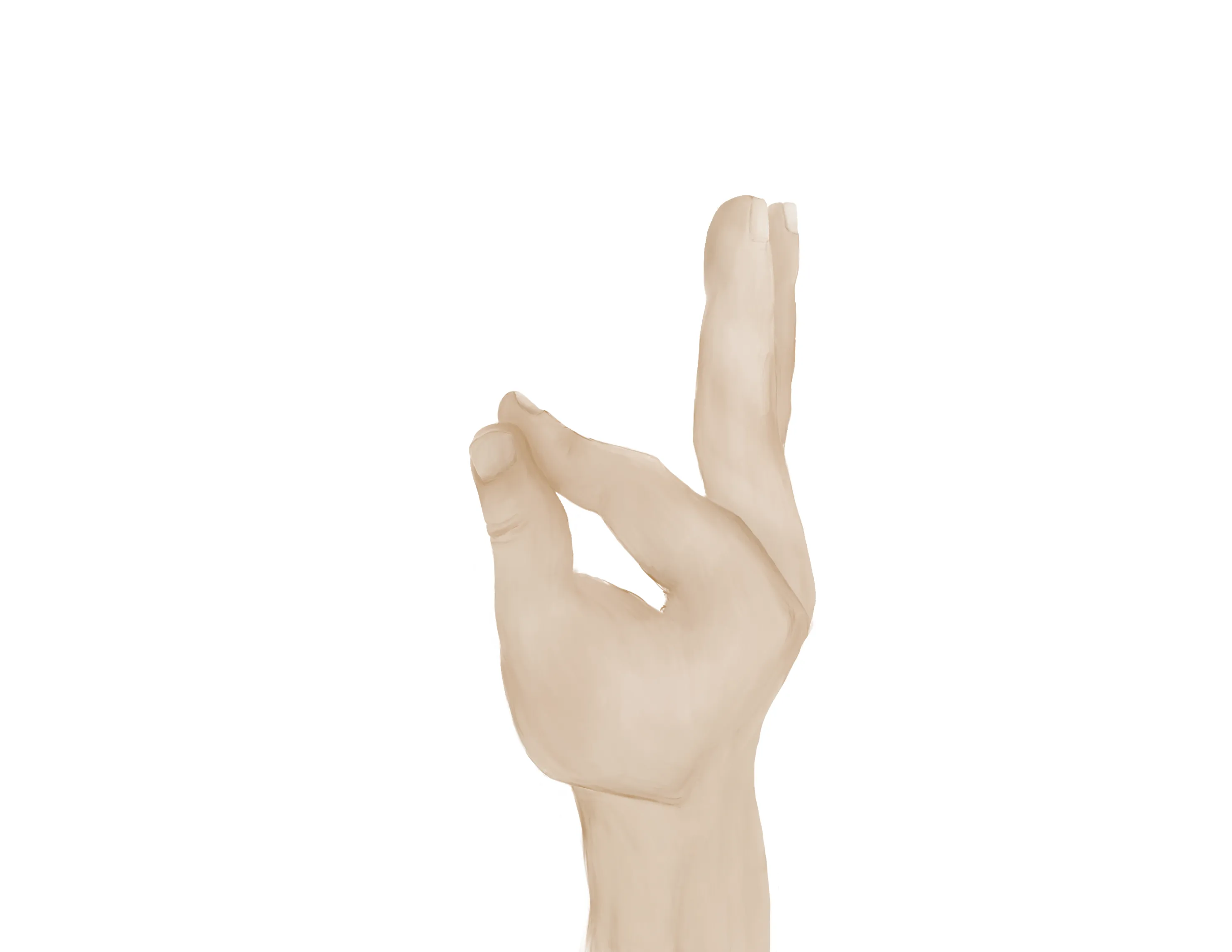
- Radial nerve/ Posterior interosseous nerve (PIN)
-

- Extension of wrist, fingers, thumb
- “Thumbs up” = PIN
- Tests extension of thumb IP and MCP joints (EPL))
- Palm on flat surface and lifting/extending thumb off the surface is also a good test for PIN (tests extension of thumb MCP joint (EPL))
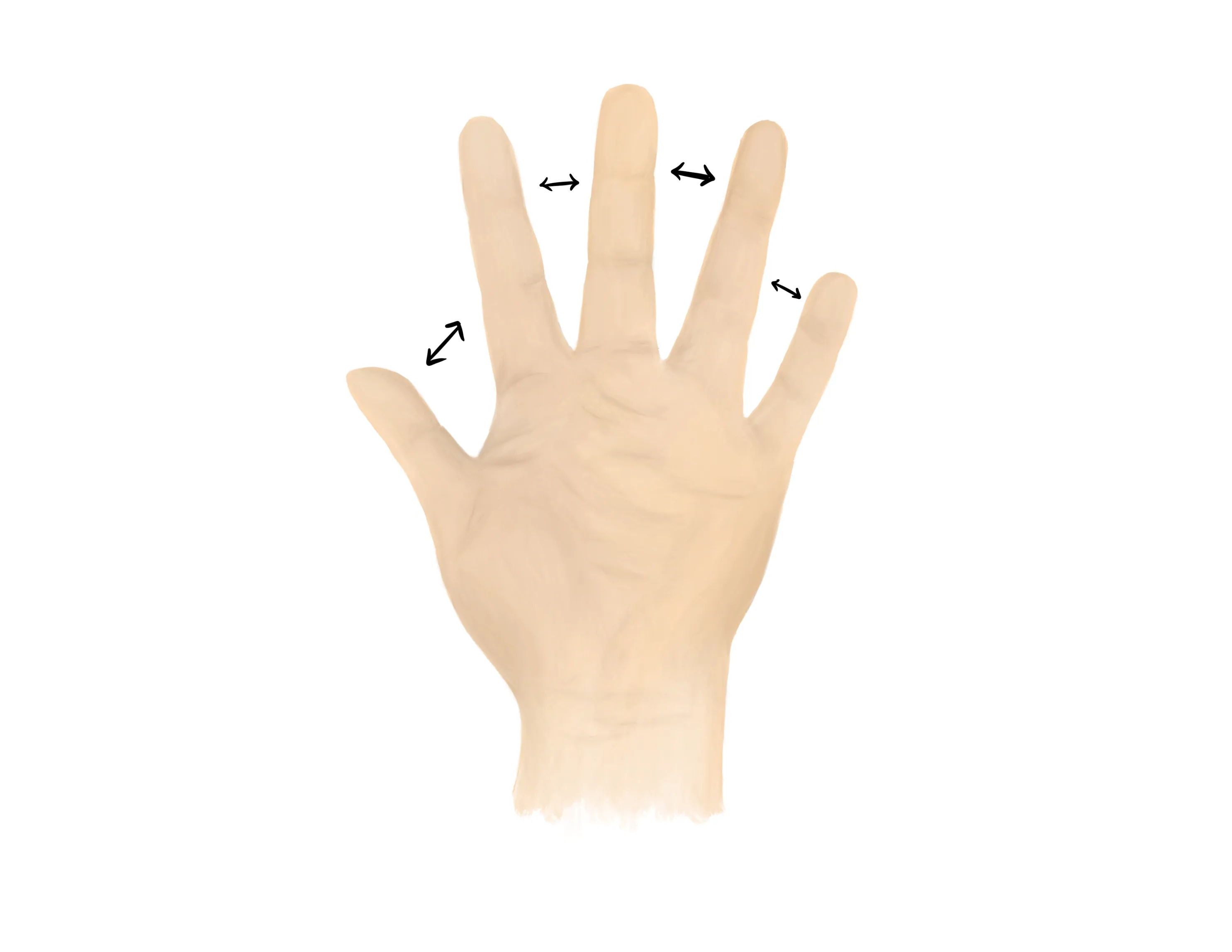
- Ulnar nerve
- Finger abduction (spread fingers, “peace sign”), finger adduction, cross fingers (“promise”)
-
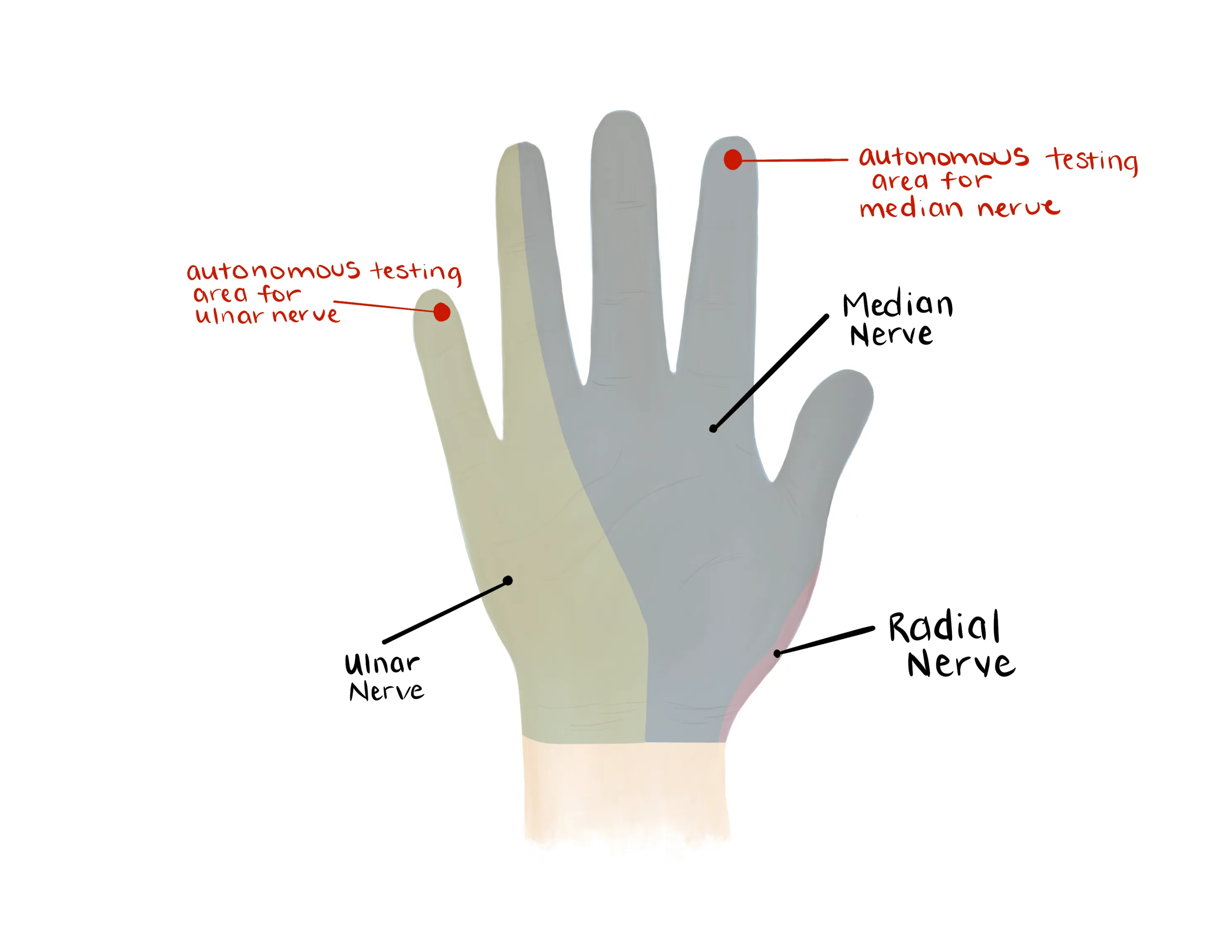
- Median, Radial, Ulnar nerve distributions
- Radial: Dorsal first web space
- Median: Volar distal index finger
- Ulnar: Volar distal small finger
-
- Distal sensation on ulnar and radial sides of the affected ray
- Two point discrimination
- Radial artery, Ulnar artery
- If having difficulty with palpation radial artery, find a doppler
- Pulse decreased - Obtain noninvasive vascular imaging and consult vascular surgery if abnormal
- Capillary refill to digits
- Will likely be pain limited
- Extension of DIPJ, PIPJ, MCPJ, Wrist
- Flexion of the DIPJ, PIPJ, MCPJ, Wrist
- Pronated PA/Lateral/Oblique of involved wrist and hand
- Injuries rarely happen in isolation, be aware of other potential carpal bone injury
- CT scan
- Helpful to delineate multiple carpal bone injuries
- Helpful for comminuted, intraarticular fracture patterns
- MRI - rarely needed in the ED
- Can be useful if there is questions about wrist instability
- Orthopaedics to order if need be
Medical Decision Making
Closed trapezium fracture :
*** is a *** y/o ***-hand dominant ***M/F with hx of *** who presents with an injury to the ***R/L hand which occurred while mechanism***, found to have a closed trapezium fracture. On exam, the patient is neurovascularly intact with well perfused digits. The injury was closed with no poke holes or punctate wounds. Radiographs reveal ***. The fracture was immobilized in a thumb spica splint. The patient will follow up in a hand clinic within one week.
Open trapezium fracture :
*** is a *** y/o ***-hand dominant ***M/F with hx of *** who presents with an injury to the ***R/L hand which occurred while mechanism***, found to have an open trapezium fracture. On exam, the patient is neurovascularly intact with well perfused digits. There was noted to be an open wound on the ***dorsal/volar aspect of the radial hand which probes to fracture. The patient was given an immediate dose of IV ancef (2/3g***). Radiographs reveal ***. Orthopaedics was consulted and the patient was made an NPO. The patient last ate ***. Orthopaedics to provide further recommendations.
Open fracture:
- Consult hand surgery (plastics vs. orthopaedics) immediately
- NPO, preop labs (type and screen, INR, aPTT, CBC, BMP)
- Ensure IV cefazolin (2-3g) were given
- Gustillo-Anderson chart for antibiotic type and dose
- Depending on the size of the soft tissue defect may require gentamicin as well
- Consult orthopaedic surgery immediately
- NPO, preop labs
- WB status: Non-weight-bearing injured hand; keep arm elevated
- Diet: Regular
- Analgesia: short course of narcotic pain medication, tylenol (scheduled)
- Ex: 5mg oxycodone q4 - 15 pills
- Immobilization
- Thumb Spica
- Maintain thumb in soda can holding position
- Disposition: Home with follow up in orthopaedic surgery clinic in 1 week
Procedure Walkthroughs:
- Position: thumb in abduction as if holding a can of soda
- Apply soft padding liberally over the thumb, wrist, and distal forearm
-

- Split the plaster/orthoglass longitudinal with its length on one side
-

- After wetting, use the split end to cocoon the first ray with the hand in the position as if holding a can of soda
- Make sure to keep plaster/Ortho-Glass off skin
Procedure Notes:
PROCEDURE NOTE Closed treatment of carpal bone fracture (excluding carpal scaphoid [navicular]); without manipulation, each bone
PRE-PROCEDURE DIAGNOSIS: fracture of the ***R/L trapezium
POST-PROCEDURE DIAGNOSIS: Same (refer above)
PROCEDURALIST: ***
ANESTHESIA: None
NAME OF PROCEDURE: Closed treatment of carpal bone fracture (excluding carpal scaphoid [navicular]); without manipulation, each bone
PROCEDURE IN DETAIL:
The risks and benefits of the procedure were discussed at length with the patient. Risks discussed included but were not limited to post-procedural pain, stiffness, numbness, and tingling. Following informed verbal consent after discussion of risks and benefits, the patient agreed to proceed with the procedure. A timeout was performed.
A well-padded thumb spica splint was applied to the injured hand. The patient's neurovascular status was consistent with baseline.
COMPLICATIONS: ***
DISPOSITION:Discharged home with follow up with orthopaedic surgery in 1 week for repeat evaluation
PRE-PROCEDURE DIAGNOSIS: fracture of the ***R/L trapezium
POST-PROCEDURE DIAGNOSIS: Same (refer above)
PROCEDURALIST: ***
ANESTHESIA: None
NAME OF PROCEDURE: Closed treatment of carpal bone fracture (excluding carpal scaphoid [navicular]); without manipulation, each bone
PROCEDURE IN DETAIL:
The risks and benefits of the procedure were discussed at length with the patient. Risks discussed included but were not limited to post-procedural pain, stiffness, numbness, and tingling. Following informed verbal consent after discussion of risks and benefits, the patient agreed to proceed with the procedure. A timeout was performed.
A well-padded thumb spica splint was applied to the injured hand. The patient's neurovascular status was consistent with baseline.
COMPLICATIONS: ***
DISPOSITION:Discharged home with follow up with orthopaedic surgery in 1 week for repeat evaluation
| Common ICD-10 Codes | Brief Description |
|---|---|
| S62.17** | Fracture of trapezium [larger multangular] |
| S62.171* | Displaced, right |
| S62.172* | Displaced, left |
| S62.174* | Nondisplaced, right |
| S62.175* | Nondisplaced, left |