Radial Head Fracture

- Usually occurs from a fall onto an outstretched hand
- Occult fractures are often identified by posterior fat pad sign on lateral X-ray
- Critical to ensure there is no mechanical block to pronosupination on physical exam
- Examining for this can be difficult due to pain at the elbow
- If concerned for mechanical block to motion and having difficulty with exam due to patient discomfort, use an intraarticular block or IV narcotics to help alleviate the discomfort and assist with exam
- Overwhelming majority of radial head fractures can be placed in a sling and discharged with orthopaedic follow-up
- Mechanism
- Usually a fall on an outstretched hand
- Radial head collides with capitellum
- Timing of injury
- Other locations of pain
- Forearm
- Associated radial/ulnar shaft fracture
- Essex-Lopresti lesion (injury to interosseous ligament and distal radioulnar joint)
- Pain distal to the fracture site should raise index of suspicion for this injury type and should be documented
- Numbness and tingling in ipsilateral UE
- Hand dominance (right vs. left hand dominant)
- Profession
Vitals
- Remove wrapping or sling to assess the skin
- Assess for deformity, bruising, edema
- Assess for tenderness at the wrist/distal radioulnar joint (DRUJ) and forearm as the energy sometime exits out the distal forearm leading to bifocal injury pattern
- Compare to normal side
- Soft tissue defect/poke hole that probes to fracture = open fracture
- Small poke hole wounds near the fracture site with a slow, continuous ooze is indicative of an open fracture
- Do not miss this and confirm antibiotics were given
- Examine the forearm compartments (soft and compressible, firm but compressible, etc.)
- Palpate the hand, elbow, arm and shoulder to identify concomitant injuries
Motor Exam:
- Axillary nerve
- Abduction of the arm
- Alternative: push elbow back into the bed/gurney
- Median Nerve/ Anterior interosseous nerve (AIN)
- Opposition of the thumb
- Opponens innervated by the median nerve - helpful to assess if concern for acute carpal tunnel syndrome
- Flexion of wrist, fingers, thumb
- “A-OK sign” = AIN
-
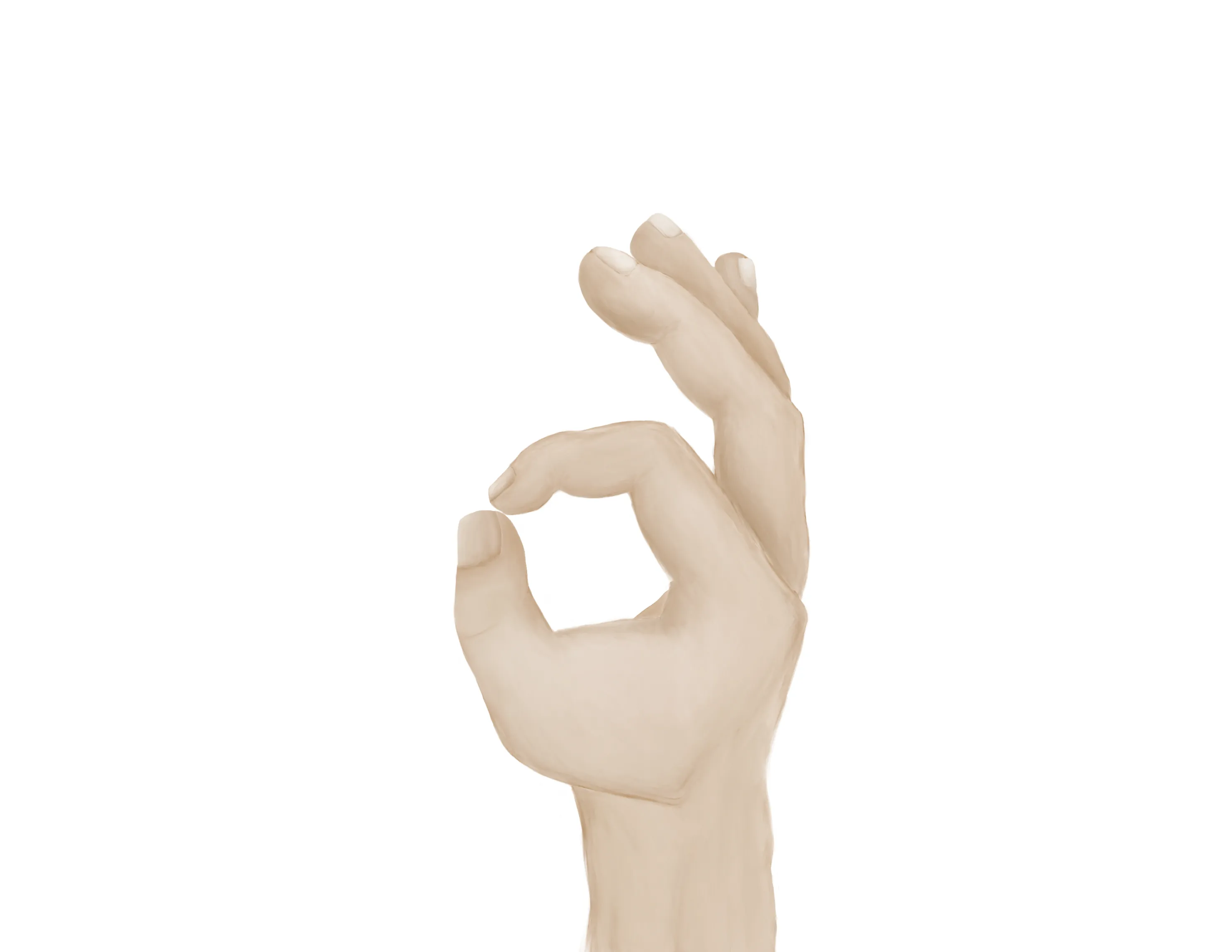
- Tests flexion of thumb IP joint (FPL) and flexion of index DIP joint (FDP)
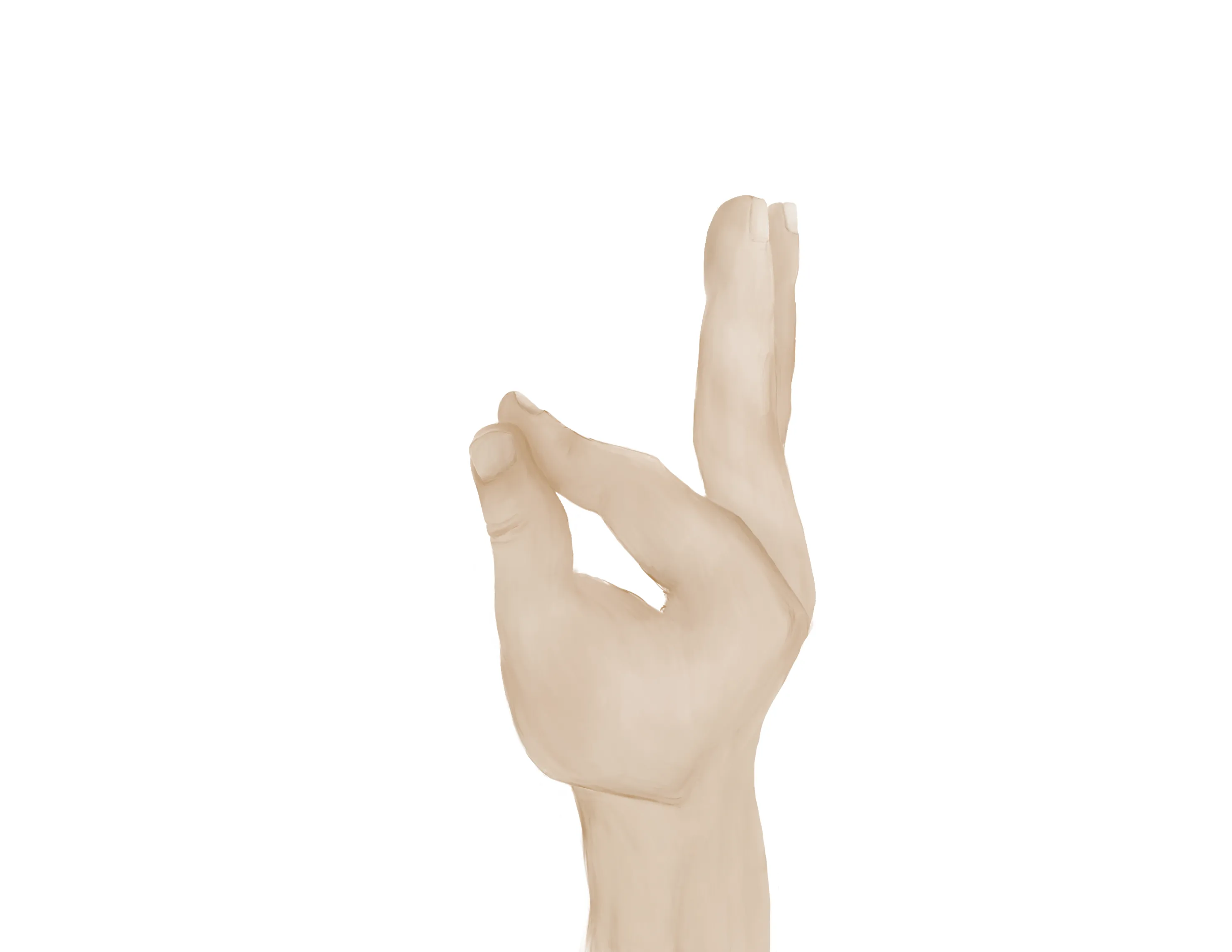
- Radial nerve/ Posterior interosseous nerve (PIN)
-

- Extension of wrist, fingers, thumb
- “Thumbs up” = PIN
- Tests extension of thumb IP and MCP joints (EPL))
- Palm on flat surface and lifting/extending thumb off the surface is also a good test for PIN (tests extension of thumb MCP joint (EPL))
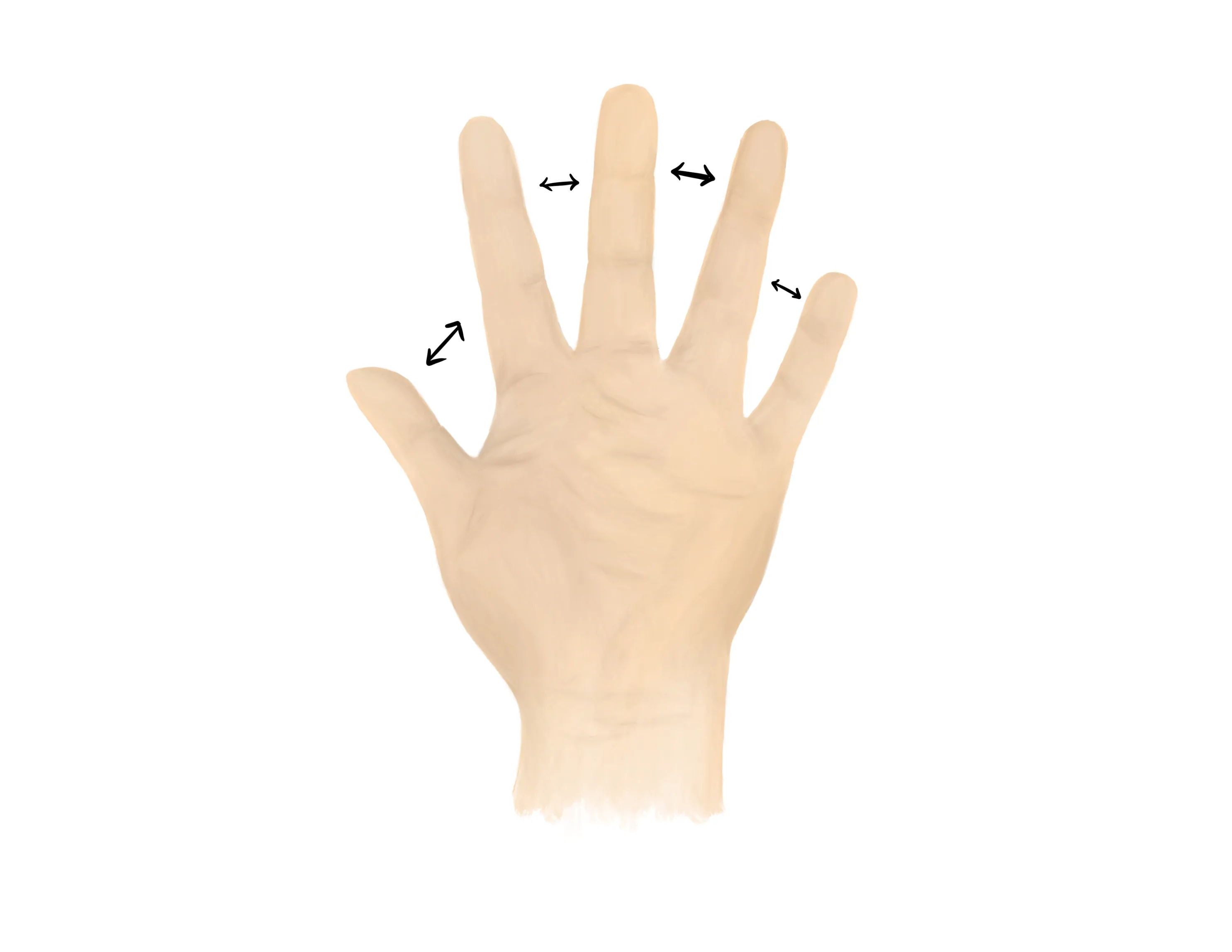
- Ulnar nerve
- Finger abduction (spread fingers, “peace sign”), finger adduction, cross fingers (“promise”)
-
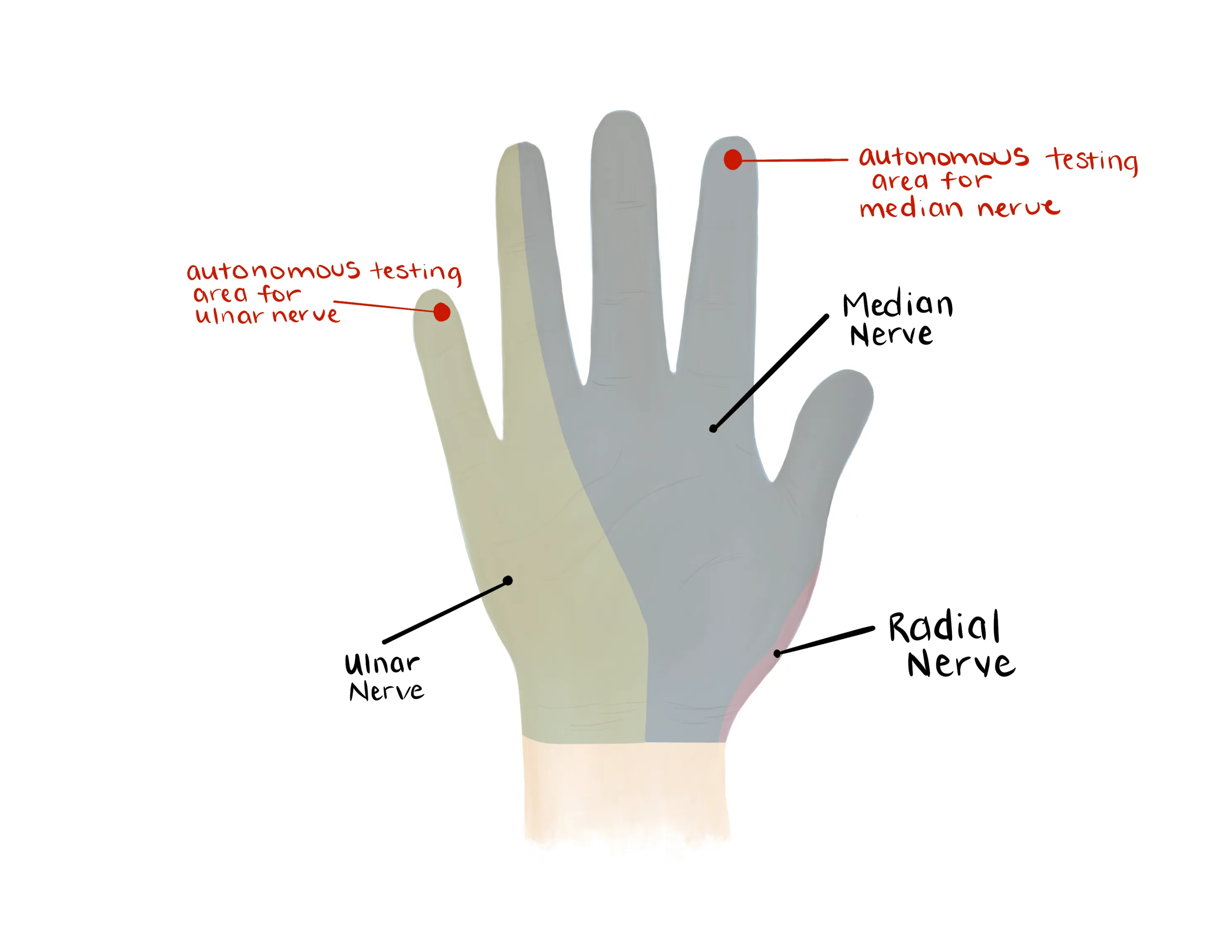
- Median, Radial, Ulnar nerve distributions
- Radial: Dorsal first web space
- Median: Volar distal index finger
- Ulnar: Volar distal small finger
-
- Radial artery, Ulnar artery
- If having difficulty with palpation radial artery, find a doppler
- Pulse decreased - Obtain noninvasive vascular imaging and consult vascular surgery if abnormal
- Capillary refill to digits
- Limited ROM at the elbow secondary to pain
- Important to assess for mechanical block to motion
- May need to give narcotic medication and/or intraarticular block during exam to assess motion
- Pronation and supination
- AP/lateral of the elbow, AP/L radius and ulnar, AP/L wrist
- Minimally displaced fractures are commonly missed
- Check for a posterior fat pad sign indicating occult fracture
-

- Radial head should always fall in-line with the capitellum on all views; if this alignment is off the radial head is either subluxed or dislocated
-

- Consider Radiocapitellar view - Greenspan view
- Oblique view with 45 degree cephalad beam
- Better view for radial head
- Sarah Image of pertinent anatomy at the elbow
- Mason Classification:
- Type 1: Nondisplaced or minimally displaced
- Type 2: Displaced fracture >2 mm, or angulated, possible block to motion
- Type 3: Comminuted and displaced, mechanical block in motion
- Type 4: Radial head fracture with elbow dislocation

Medical Decision Making
Closed Radial Head Fracture:
*** is a *** y/o ***R/L hand-dominant individual with a history of *** presenting with an injury to the *** elbow which occurred while ***, found to have a closed radial head fracture. On exam, the patient is neurovascularly intact with no poke holes or punctate wounds. There is tenderness to palpation and localized edema about the fracture site. Radiographs reveal ***, with a posterior fat pad sign. The elbow was immobilized in a sling and will follow up with orthopedic surgery in one week.
Open Radial Head Fracture:
*** is a *** y/o ***R/L hand-dominant individual with a history of *** presenting with an injury to the *** elbow which occurred while ***, found to have an open radial head fracture. On exam, the patient is neurovascularly intact with a laceration about the lateral elbow which probes to the fracture. There is tenderness to palpation and localized edema about the fracture site. The patient was immediately given a dose of IV ancef/gentamicin***. Radiographs reveal ***, with a posterior fat pad sign. Orthopaedics was consulted for further management. The patient was made npo and last ate at ***.
If open fracture or traumatic arthrotomy:
- Consult orthopaedic surgery immediately
- NPO, preop labs
- Ensure IV antibiotics were given (ancef, gentamicin)
- Gustillo-Anderson chart for antibiotic type and dose
- WB status: Nonweightbearing injured upper extremity
- Diet: Regular
- Analgesia: short course of narcotic pain medication, tylenol (scheduled)
- Ex: 5mg oxycodone q4 - 25 pills
- Immobilization
- Sling immobilization
- Disposition: Home with follow up in orthopedic surgery clinic in 1 week
| Common ICD-10 Codes | Brief Description |
|---|---|
| S52.12 | Fracture of head of radius |
| S52.121 | Displaced fracture of head of right radius |
| S52.122 | Displaced fracture of head of right radius |
| S52.124 | Nondisplaced fracture of head of right radius |
| S52.125 | Nondisplaced fracture of head of left radius |
