Compartment Syndrome of the Hand
- Condition in which the circulation within an anatomic compartment is compromised due to increased pressure within the compartment causing ischemia and infarction of vital structures
- This is a CLINICAL DIAGNOSIS and an orthopaedic emergency
- May result from a decrease in the compartment size (e.g. tight dressing, cast, etc.) and/or increase in fluid volume in the compartment (e.g. swelling from crush injury or fracture)
- While not as common as forearm compartment syndrome, hand compartment syndrome is not rare
- Mechanism
- Crush
- Fracture
- Snake bite
- Hemophilia
- Burns (circumferential eschar)
- Tight external wrapping
- Extravasation from IV infusion
- Local anesthetic blocks
- Timing of injury
- Early diagnosis and prompt surgical intervention is essential to prevent severe complications and permanent tissue death
- Classic 5 P’s
- Pain
- Most sensitive/early
- Out of proportion to the injury and increasing
- Worse with passive stretch
- Paresthesias
- Numbness and tingling is a sequela of the injury or compartment syndrome
- Late sign of compartment syndrome
- Pulselessness → Late finding
- Paralysis → Late finding
- Pallor → Late finding
- Anticoagulation
- Timing of last dose
- Last time patient last ate (NPO status)
Vitals
- If intubated/sedated/obtunded and unable to give exam, notify orthopaedics immediately for likely Stryker Pressure Manometer measurement
- If intubated/sedated/obtunded and unable to give exam, notify orthopaedics immediately for likely Stryker Pressure Manometer measurement
- Remove any splint/wrapping
- Basic appearance (swelling, bruising, deformity)
- Hand can be tense, swollen, and held rigid in a flexed position
- Assess skin about the fracture site
- Can have a compartment syndrome with an open fracture
- Ensure IV antibiotics are administered, if open
- Palpate compartment (soft, firm but compressible, firm and noncompressible)
- 11 Hand Compartments
- Thenar
- Midpalm
- Hypothenar
- 4 dorsal interosseous
- 3 palmar interosseous
- Adductor pollicis
-

- Distract the patient and passively flex/extend fingers and wrist
- Worsening pain with passive stretch of the fingers is very concerning for compartment syndrome
- This exam maneuver is good gauge if concerned about drug seeking behaviors
- Rapidly increasing narcotic requirement for pain control should trigger concern for compartment syndrome but may be difficult to differentiate from drug seeking behaviors
Motor Exam:
- Median Nerve/ Anterior interosseous nerve (AIN)
- Opposition of the thumb
- Opponens innervated by the median nerve - helpful to assess if concern for acute carpal tunnel syndrome
- Flexion of wrist, fingers, thumb
- “A-OK sign” = AIN
-
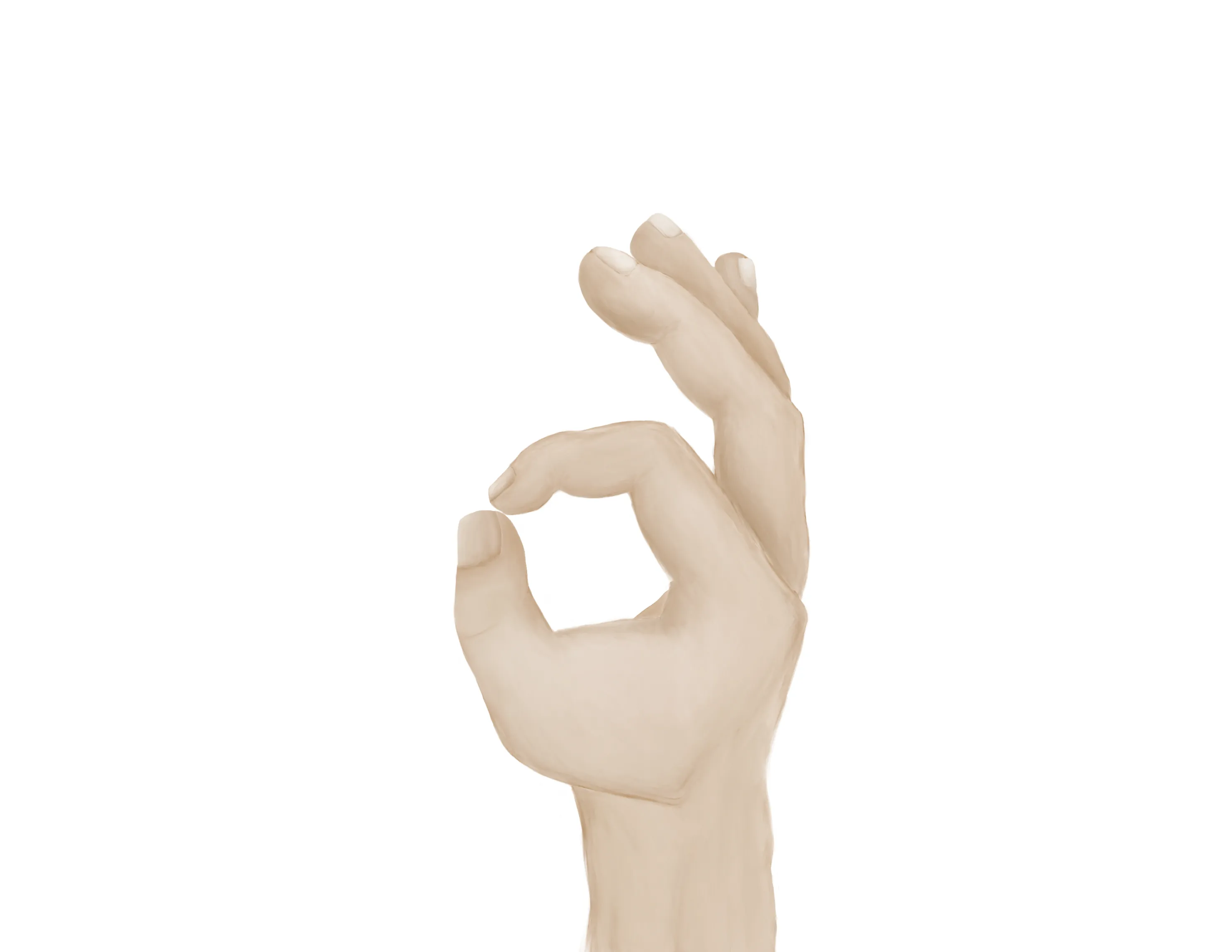
- Tests flexion of thumb IP joint (FPL) and flexion of index DIP joint (FDP)
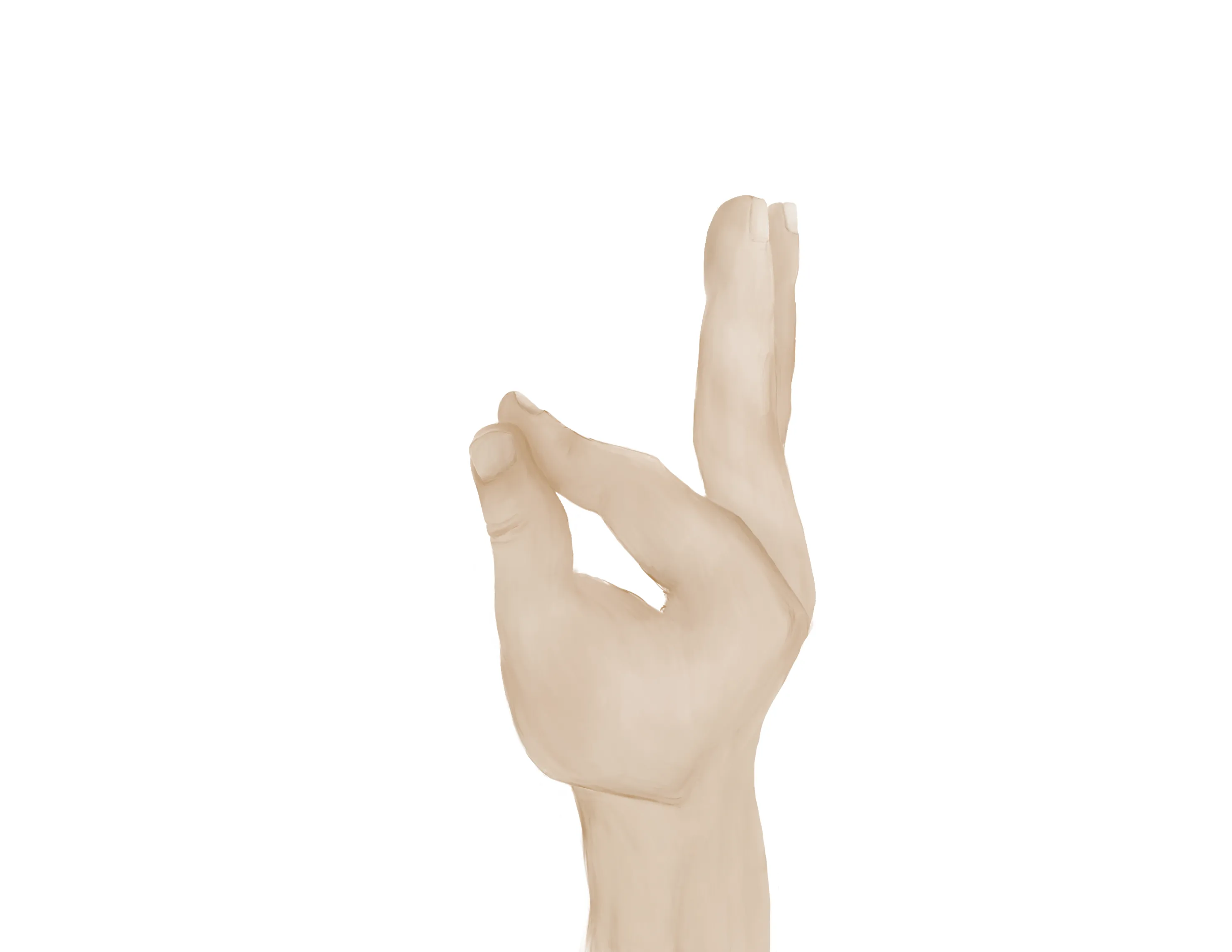
- Radial nerve/ Posterior interosseous nerve (PIN)
-

- Extension of wrist, fingers, thumb
- “Thumbs up” = PIN
- Tests extension of thumb IP and MCP joints (EPL))
- Palm on flat surface and lifting/extending thumb off the surface is also a good test for PIN (tests extension of thumb MCP joint (EPL))
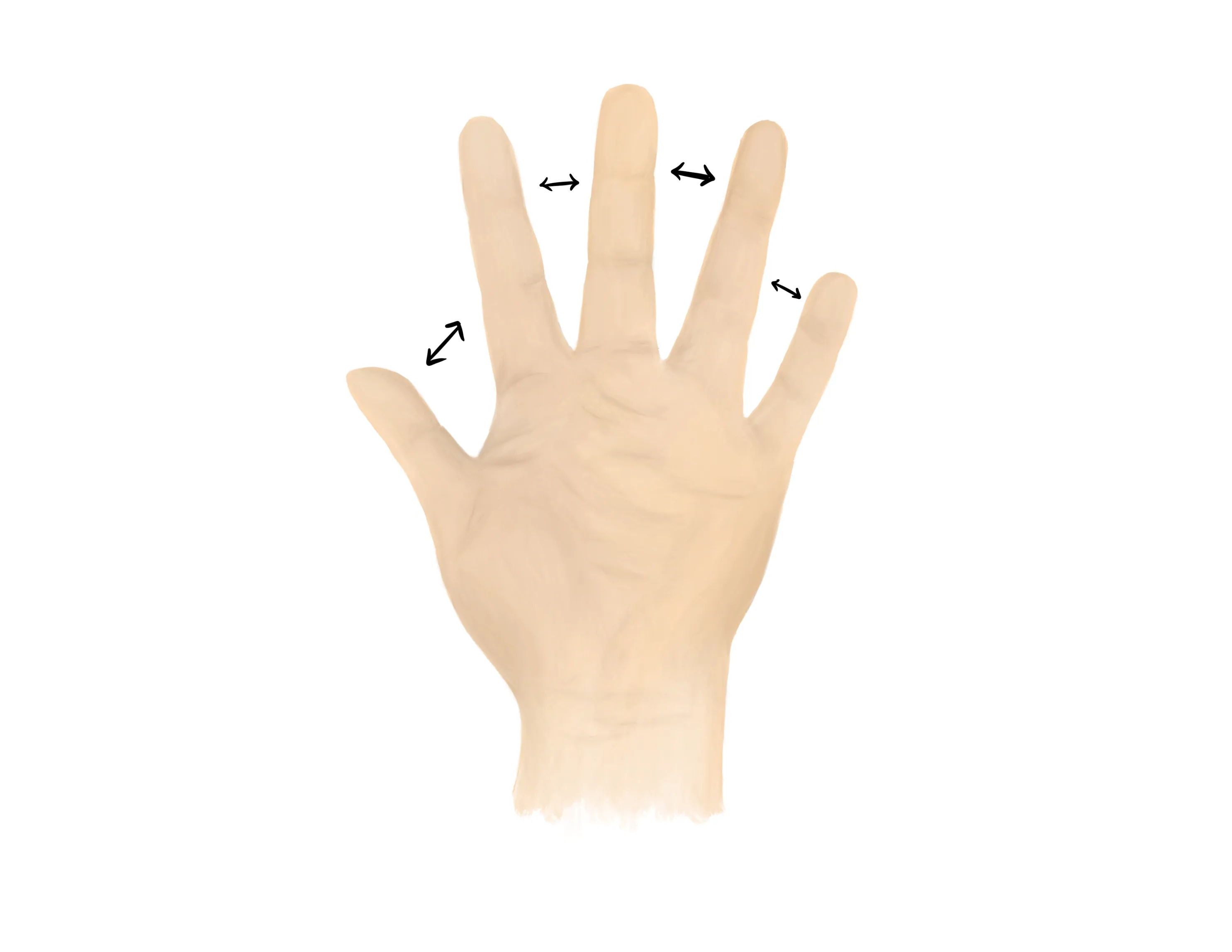
- Ulnar nerve
- Finger abduction (spread fingers, “peace sign”), finger adduction, cross fingers (“promise”)
-
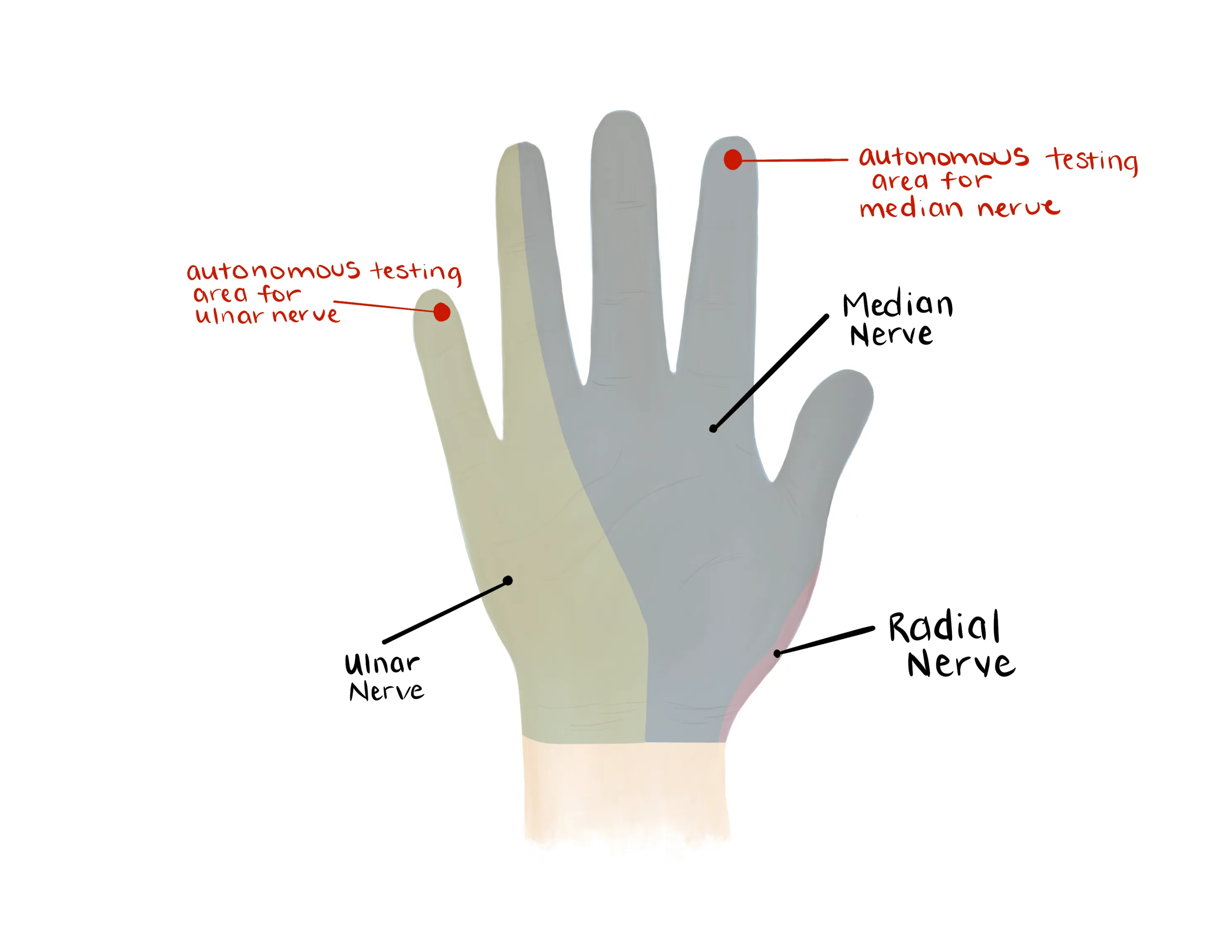
- Median, Radial, Ulnar nerve distributions
- Radial: Dorsal first web space
- Median: Volar distal index finger
- Ulnar: Volar distal small finger
-
- Radial artery, Ulnar artery
- If having difficulty with palpation radial artery, find a doppler
- Pulselessness is a late finding
- Capillary refill to digits
- Pain with passive or active movement of the digits is concerning for compartment syndrome
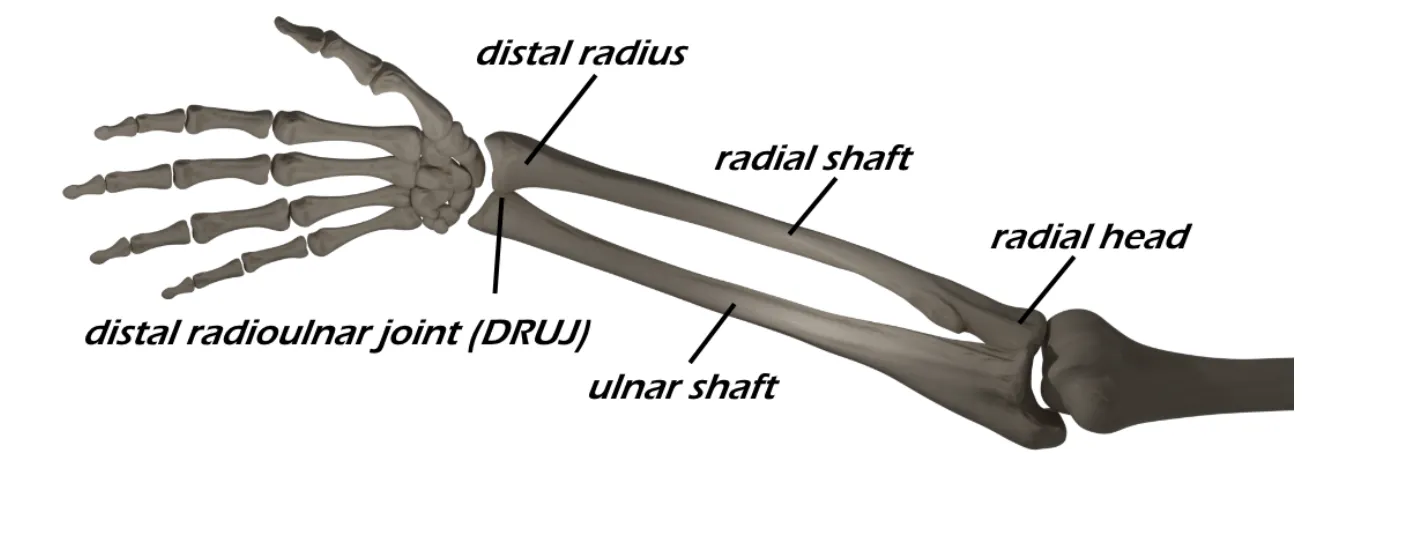
- AP / Lateral / Oblique of the hand
- Fracture is most common etiology for compartment syndrome
- Compartment syndrome can occur with open fractures
Medical Decision Making
Concern for Hand Compartment Syndrome:
*** is a *** y/o ***R/L hand-dominant individual with a history of *** with progressively worsening pain and swelling of the ***R/L hand and increasing narcotic requirement, concerning for compartment syndrome. On exam, the patient is neurovascularly intact with tense and swollen compartments of the hand. There is worsening pain with passive stretching of the digits. Radiographs reveal ***. Orthopaedics was consulted for further evaluation. The patient is npo and last ate ***.
- Consult hand surgery immediately
- WB status: Non weight bearing injured hand, aggressive elevation
- Diet: NPO
- Analgesia: oral narcotics with IV for breakthrough
- Monitor for increasing narcotic need which is often a clue for developing compartment syndrome
- Immobilization
- Immobilization should be removed to assess the soft tissues, pulses, etc. and decrease external circumferential compression
- Disposition: Pending hand surgery assessment
| Common ICD-10 Codes | Brief Description |
|---|---|
| T79.A1 | Traumatic compartment syndrome of upper extremity |
| T79.A11 | Traumatic compartment syndrome of right upper extremity |
| T79.A12 | Traumatic compartment syndrome of left upper extremity |
| M79.A1 | Nontraumatic compartment syndrome of upper extremity |
| M79.A11 | Nontraumatic compartment syndrome of right upper extremity |
| M79.A12 | Nontraumatic compartment syndrome of left upper extremity |